

Nose Revision (Revision Rhinoplasty) creates a smoother and more natural looking nose, which will even work to heal your mind.
You need to undergo revision rhinoplasty (nose surgery), if you are experiencing any of the following cases: your nose shape is different from what you expected after rhinoplasty (nose surgery), you have an excessively high bridge after rhinoplasty (nose surgery), the tip of your nose is excessively sharp, seriously shifting implant or implant transparency and your nose implant is collapsed or you have an inflamed nose after rhinoplasty (nose surgery).
Revision rhinoplasty (nose surgery) requires much more advanced techniques and experience than rhinoplasty (nose surgery) so you are advised to get revision rhinoplasty (nose surgery) from our well-experienced surgeons.
Some patients unhappy with a previous rhinoplasty from another clinic find it difficult to imagine having revision surgery, having already ‘given up’ on achieving the nose that they want.
Some patients may find themselves feeling depressed with their appearance and uneasy about the prospect of risking surgery once more.
However, at JW Plastic Surgery, we strongly encourage all patients considering revision rhinoplasty to regain their confidence and trust that a revision surgery can and will bring them the results that they wish for!
Whatever your reasons for wanting to receive revision rhinoplasty, we recommend a patient to get this surgery within 1~2 weeks after their primary rhinoplasty(nose surgery). Otherwise, he or she may have to wait at least 6 months (even over 1 year depending on your health condition) before undergoing extensive surgery. The reason for these few months of waiting are to give enough time until your nose tissue have calmed and have become soft.
There are several scenarios when you should take revision rhinoplasty right after the primary rhinoplasty(nose surgery), which are as follows:

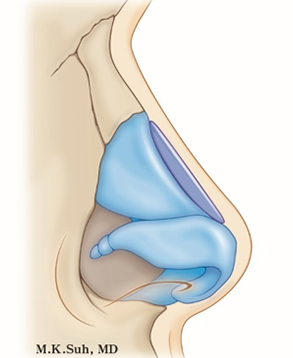
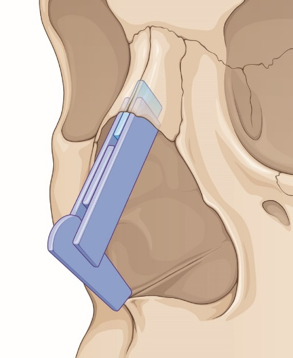
We will remove the slant implant, which doesn’t fit to your nasal base, and the readjusted implant will be inserted into your nose. However, if your nasal skin became thin, then we will operate by returning your nasal skin to its original thickness. The thin skin will be augmented with dermis, corium or fascia.

The implant will be movable if it’s inserted under the skin layer and not under the fascia of the nasal bone. It can be corrected by precisely re-positioning the implant under the fascia. However, if the fascia is already damaged that won’t be able to hold the implant tightly. Goretex or autologous materials can be used to prevent movement instead of Silicone.

The implant can become visible due to skin thinning. We reinforce the thin skin by dermis (or artificial dermis) or Fascia. If the condition of the nose has become bad, we would remove the silicone and use only autologous materials (dermo fat) or cartilage to heighten the nasal bridge.

The skin turning red or white is due to poor blood circulation that is caused by skin thinning. If this condition is not corrected quickly, the skin will get thinner and the silicone inside can penetrate the skin. We would remove the silicone or cartilage causing this problem and correct the thin skin of dorsum and tip by reinforcing it with artificial or autologous dermis.

The contours of an implant can become visible due to the difference between the width of the implant and the width of the nasal bone base. We would change the silicone to a suitable one and reinforce the stretched and weaken skin of the nasal bridge by dermis, artificial dermis or fascia.

For upturned nose surgery, using either cartilage grafting techniques of nasal septum or rib cartilage grafting techniques can bring a very positive result. This surgery releases the agglutination between all scarred tissues and separates the capsular tissues, pulls the cartilage of the nasal tip downwards to a proportional length and position, and fixes the tip through use of nasal cartilage or rib cartilage.

The demarcation of the implant on the bridge of the nose is sometimes distinctive, especially when smiling. We revise this situation by extending the length of the detached implant from the nose and grinding the tip of the implant to be thinner in order to not to give a burden on the tip of the nose.
It is impossible to thoroughly remove illegal substances, however, we try our best to remove the substances to the maximum extent possible. Then we operate by using of autologous cartilages, usually using dermis fat or chest cartilage.
The level of the surgery is determined based on the conditions of the diffusibility of illegal substances. This surgery involves an advanced level of operation and requires an abundance of experience and expertise. You are advised to receive this surgery from a well-experienced and skilled surgeon.
Many individuals have received injections of illegal substances injection from quack doctors (illegal doctors or not certified plastic surgeons). These practices were prevalent in the past, but still occur even today. Even though the quacks (illegal doctors or not certified plastic surgeons) say that they use collagen or botox injections, they actually use silicone or paraffin injections. Both silicone and paraffin can easily be spread to your tissue once these are injected into your body, thus it is very difficult to remove them. Although you don’t see any problems initially after the illegal injection, the side effects can suddenly occur a few years or tens of years later. You should never receive any of these kinds of injections of illegal substances. The side effects include inflammation, discoloration of skin, tissue necrosis, falling out of illegal substances, causeless headaches, and more.
It is possible that the bridge of the nose reverts back to an hump nose or the nasal tip turns low or becomes slanted.
We operate by cutting the muscle (depression of nose tip muscle), which pulls down the nasal tip, inside of the short nasal columella.
Your nose can have a deep set as a result of excessive removal of nasal bone or nasal cartilage during rhinoplasty. This sunken area can be filled with autologous of cartilage or dermis transplantation.
In case the implant is filled up to the nasal tip, you can’t make a pig-like nose or the nose tip becomes rigid. It is important to maintain the natural nasal tip and for this, any kinds of implants should never be inserted up to the nasal tip.
Silicone allergy would be a rare occurrence. The allergic reaction can appear as swelling of nasal tip or glabella; repeated swelling and decreasing; the swelling area becomes soft and mushy; and the surgical areas turn to red. In these cases, the silicone in your nose should be removed and replaced with safe new materials or autologous.
This refers to an upside-down V-shaped indentation between the end of the nasal bones and the start of the upper lateral cartilages, along the top of the bridge. The main cause of inverted V deformity is the result of following hump removal in rhinoplasty, the upper lateral cartilages has fallen against the septum and this valve has become significantly narrowed. Other than this reason, most other cases are the result of wounds. This can be corrected by transplanting cartilage of nasal septum.
Saddle nose refers to sunken nasal bridge (lower 1/3) from loss of septal support.
The saddle nose exists in a wide spectrum from minimal depression to severe collapse. Depending on the severity, the treatment option can range from simple camouflage technique to structural reconstruction using rib cartilage.
If the side cartilage of the nose collapses during inspiration (breathing in), it causes breathing difficulties as the nostril is being blocked. This surgery is performed for nose function rather than aesthetic purposes. To raise the drooping tip of the nose, a part of the ear-cartilage is implanted to provide nasal tip support.
The height of the nose bridge can be readjusted if a patient is dissatisfies for a personal reason. It is a comparably easy and simple operation amongst other revision rhinoplasty surgeries.
Some individuals prefer a straight-edged shape of nose and some others prefer a turned-up nose.
If a patient isn’t satisfied with his/her profile line shape of their nose, by simply readjusting the implant, the correction can be conducted. However, some cases have to be accompanied with the surgery of raising or lowering of nasal tip.
Some people may have septal deviation or turbinate problem. The diagnosis of a deviated septum can be made by your doctor. Your doctor will perform a thorough evaluation of your symptoms and will examine your nose. We straighten the cartilage and bone that have led to the septum being deviated.
The turbinates are made of bone and soft tissue. Either the bone or the soft tissue can become enlarged. In most patients, enlargement of the soft tissue part of the turbinate is the major problem when the turbinates become swollen. When the turbinates are large, they are called hypertrophic turbinates. We shrink the size of turbinates to improve nasal obstruction.
Internal nasal valve is the specific slit-like segment between the septum and the caudal margin of upper lateral cartilage. Insufficiency of this valve can be caused by high septal deviation, mucosal scarring, and upper lateral cartilage collapse.
Several techniques including spreader graft are available to correct incompetence of internal nasal valve.
The external valve occupies a greater volume of space compared to the internal valve.
Excessive resection of cartilage during tip plasty can easily lead to external valve collapse.
The operative techniques to correct this problem are alar rim graft, alar batten graft, lateral crural onlay graft, and lateral crural strut graft.
Pinched tip is an unaesthetic appearance of nasal tip characterized by excessively narrowed tip, deep alar groove extending to the alar rim, shadowing between the lobule and ala, and ball-shaped tip.
Pinched tip is caused by weakness, collapse or malposition of lower lateral cartilages. This deformity may be congenital or secondary to prior rhinoplasty or trauma.
A pinched tip not only represents an aesthetic problem but can also be associated with functional problems such as difficulty in breathing due to external nasal valve collapse.
Pinched tip deformity can be corrected using cartilage batten graft, alar rim graft, or lateral crural graft.
Asymmetric nasal tip after an unsuccessful rhinoplasty is always accompanied by columella deviation and nostril asymmetry. Correction techniques vary according the underlying causes.
The nasal tip revision requires diverse surgical experiences and skills of surgeon.
JW makes every single preoperative preparation on the same day of the operation for our customers’ convenience.
JW nose team constitutes 2 nose specialists with know-how from various clinical experiences, as well as dedication to achieving the best result by medical research.












")
{kind=link}
{kind=link}
{kind=link}
{kind=link}